[page 444]
APPENDIX M
THE REORGANISATION OF THE NATIONAL HEALTH SERVICE AND THE CENTRAL DEPARTMENTS
Background to the Reorganisation
1. There were three main reasons for the introduction of the National Health Service in 1948. The first was that many people were experiencing great difficulty in finding the money to pay for medical treatment. Second, the hospital services were running into serious financial trouble. (This was not just a matter of too few beds and too many of these unsatisfactory, but also because there were two separate systems of administration - voluntary hospitals and local authority hospitals.) Third there was a need to remedy the uneven distribution of staff and other resources between different geographical areas and between different parts of the services.
2. To deal with these problems a unified service was needed and had been intended, but for political reasons and because health services had grown up that way, the NHS was saddled with a tripartite structure. In one part were the hospital and specialist services. In another were the general practitioner services, administered by autonomous Local Executive Councils. In the third part were the local authority health services administered by the major local authorities. This division of responsibility led to lack of balance, overlap and deficiencies in the services, particularly in services for children, old people and people with mental illness, mental handicap or physical handicap. On the hospital side the services for these groups had failed to attract the financial and other resources they needed, while on the local authority side complementary domiciliary and community services had been slow to develop and were developing unevenly. For these and other reasons the framework of the NHS was re-designed and on 1 April 1974, a new administrative structure was introduced under the NHS Reorganisation Act (1973).
Outline of the reorganised administrative structure
3. The stated purposes of the change were to unify the local administration of health services under new Area Health Authorities; to base the day-to-day running of the services on Districts, each planned to provide comprehensive health services for a population of about a quarter of a million; to provide for collaboration between the NHS and certain related services for which local authorities still remained responsible; to give full weight to the views of the health professions in the planning and management of services; to correct disparities among regions and among specialties; and to provide a new means of representing the interests of the public in the health services at district level. The services brought together under Area Health Authorities were hospital and specialist services previously administered by Regional Hospital Boards, Hospital Management Committees and Boards of Governors of teaching hospitals; the personal health services previously administered by local authorities through their health committees (health visiting, home nursing, maternal and child health care, vaccination and Immunisation, health centres etc.); and the school health services previously administered by local authorities through their educa-
[page 445]
tion committees. Details of the new structure are set out in "Management Arrangements for the Reorganised National Health Service", in "Management Arrangements for the Reorganised National Health Service in Wales" and in a wide range of DHSS and Welsh Office circulars. A summary of the arrangements is provided in what follows.
4. Area Health Authorities. These are the key authorities with boundaries drawn to correspond with matching local authorities. The chairman of the Authority is appointed by the Secretary of State, and the members by the matching Local Authority and by the Regional Health Authority (see below), after consultation with the professions and interested organisations. The AHA is responsible for planning and developing health services in its Area in relation to national policies and regionally determined strategies and in co-operation with the matching Local Authority. It allocates resources between districts and monitors the performance of the districts in relation to agreed plans. It is accountable to the RHA (in Wales there is no Regional Authority interposed between the AHA's and the Welsh Office - the central government department). The AHA is advised by an Area Team of Officers (Area Medical Officer, Nursing Officer, Treasurer and Administrator).
5. Family Practitioner Committees. The reorganisation has left unchanged the status of general medical and dental practitioners, ophthalmic medical practitioners, opticians and pharmacists. All continue to provide services as independent contractors under contracts administered by Family Practitioner Committees. AHAs have a statutory duty to set up FPCs. There is some cross-membership and a close working relationship is essential, but the FPC has sole responsibility for matters which relate to the administration of contracts with practitioners. The AHA is responsible for matters involving the planning of practice services, the development of health centres and arrangements for nurses (including health visitors) and other skilled staff employed by the AHA to work with general practitioners but the AHA will have the advice of the FPC. The AHA has to ensure that any plans affecting contractor services are acceptable to the FPC.
6. District Management Teams. Except in one-district Areas, the day-to-day running of the NHS is based on Districts. The District is not a separate tier of the administrative hierarchy but part of the Area administration so organised as to enable the AHA to meet community needs most effectively. The members of each District Management Team (District Community Physician, Nursing Officer, Finance Officer, Administrator and a consultant and general practitioner) are jointly responsible to the Area Health Authority (but are not accountable to the ATO, except in Wales) for most of the NHS services in their district. They assess existing services in the district, identify unmet needs, suggest priorities and draw up plans for the approval of the AHA. Within each district there is a District Medical Committee to represent all general medical practitioners and hospital specialist staff and to coordinate
[page 446]
medical aspects of the health services throughout the District. The views of the consumer of the district health services are represented by Community Health Councils.
7. Joint Consultative Committees. Four important health related services lie outside the NHS and are the responsibility of local government authorities: personal social services; educational services; housing; and environmental health services. Collaboration between the authorities responsible for these services and the health authorities is essential. To achieve this Joint Consultative Committees have been set up by Area Health Authorities and matching local authorities to advise on the planning and operation of services of common concern.
8. Regional Health Authorities. The principle role of the regional authorities is to develop strategic plans and priorities based on a review of the needs identified by the AHAs within its boundaries and on its judgement of the right balance between those areas' claims on its resources. In this role it is guided by national policies. It is also responsible for identification and provision, directly or through its AHAs, of services that need a regional approach such as arrangements for the less common specialties (eg neurosurgery, cardiac surgery, radiotherapy). Each RHA has at least one University Medical School within its boundaries and has a special responsibility for the service facilities needed to support undergraduate and postgraduate medical and dental education. In Wales there is no RHA.
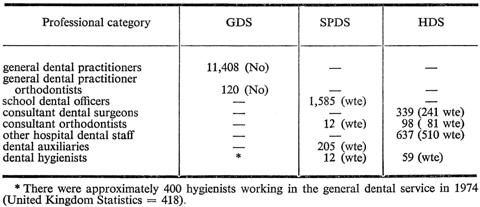
9. Dental Services. The administrative structure of the Dental Services in the reorganised NHS follows a pattern intended to be comparable with that in medicine (ie the service is two-tiered with a tier at Regional and a tier at Area level and a central government department). It was originally proposed that there should be administrative Regional Dental Officers, Area Dental Officers and part-time District Dental Officers. In the event, no Regional Dental Officers and very few (only 45) District Dental Officers have been appointed but all Area Dental Officers are now in post. There is no comparable district dental committee: the interests of general dental practitioners are represented on the Area Dental Committee. Since reorganisation, the School Dental Service has been the responsibility of Area Health Authorities and the DHSS (the Welsh Office in Wales): prior to 1974, it was that of the local education authorities and the DES.
10. Department of Health and Social Security. The Secretary of State is responsible to Parliament for the administration of the NHS and in carrying out this task is assisted by the Department of Health and Social Security. That responsibility includes establishing national policies and priorities; agreeing with regions and areas on the objectives to be developed in the light of those policies and priorities; allocation of resources to enable regional authorities to put their plans into effect (family practitioner services are provided for separately and are not in-
[page 447]
cluded in regional and area budgets); development of the resources essential to the services (personnel, finance, property, supply); certain types of research; and the preparation of national statistics. Expert advice is available to the Department from a structure of advisory bodies.
The Welsh Office
11. The administrative structure of the health services in Wales differs from that in England in a number of respects. The most important of these is that there is no regional health authority. This means that the Welsh Office (the central government department) is itself responsible for strategic planning within the Principality and for monitoring the performances of the eight AHAs. The Secretary of State for Wales is directly responsible for all services for children and this includes the appropriate social services, primary and secondary education and housing as well as services within the National Health Service. Because there is no regional authority, substantially more planning and decision making responsibilities are delegated to the AHAs than in England. A special body, the Welsh Health and Technical Services Organisation, is responsible amongst other things for the design and execution of major capital works, the systematic evaluation of contracting arrangements for supplies, and for a computer-based management information service.
The Department of Health and Social Security
12. Although some of the health needs of children are met by elements of the NHS devoted exclusively to them - eg school health services and children's departments in general hospitals - many other needs are met by personnel and facilities shared with adults - eg ENT surgeons, GPs (medical and dental), diagnostic laboratory services and health centres. Children do not have a separate health service, they are clients of the NHS provided for the population at large. Similarly, local authority social service departments provide services for people of all ages, there is no separate management structure for their services for children. But both the NHS and social service departments provide specialised services and institutions for children and employ professional staff who specialise in the needs of children - eg community medical services for children, services for the residential care and fostering of children, consultant paediatricians and Specialists in Community Medicine (Child Health).
13. At the end of 1972 the headquarters of the Department of Health and Social Security was reorganised and a new Service Development Group was established. This group includes six divisions, three of which are concerned with the development of services on a "client group" basis, namely: Services for the Socially Handicapped, Services for Mental Health and Children's Division. The new organisation recognises that most of the Department's work requires several disciplines to act in partnership and provides professional groups alongside administrative divisions with related but direct responsibilities. Thus groups of medical, nursing and social work
[page 448]
service officers are associated with the Children's Division and are responsible between them for central oversight of NHS and PSS services provided exclusively for children. They do not take the lead in developing policy for the services which children share with adults. For these, the object is to provide advice to other divisions and groups on the special needs of children. For example mentally handicapped children in long-stay hospitals need specialised medical and caring services along with mentally handicapped adults. Yet as children they have other needs best met by child-oriented services. The two sets of needs are closely linked. When a problem arises for which particular expertise in mental handicap is required, the lead is taken by the Mental Health Division. The Children's Division takes the lead on those problems which arise directly from the fact that the patients are children (eg the provision of paediatric care and issues concerning such matters as play, recreation and parental visiting).